

WHAT’S AILING MEDICINE?


Cardiologist Sandeep Jauhar, director of the Heart Failure Program at Long Island Jewish Medical Center, is a reluctant physician. Well, in some ways. Also an author and a New York Times columnist, Jauhar loves medicine, but he hates that we’ve ended up with dissatisfied patients, unhappy doctors, and a dysfunctional health care system.
You’d be wrong to think that Doctored: The Disillusionment of an American Physician (Farrar, Straus and Giroux) by Sandeep Jauhar is a long, whiny complaint or an angry screed in which he wants to fight a turf battle and offer his “visionary” solution to our health care woes. Doctored is, in fact, a probing memoir that often reads like a novel. It’s a worthy—if sobering—sequel to his well-received Intern: A Doctor’s Initiation, and the two books together would make a nice, useful gift for any would-be or hope-to-be doctor.
After abandoning a promising career as a physicist in his mid-twenties, Jauhar set out to become a doctor. His debut book (Right) focuses on the first year of his arduous residency at a top teaching hospital in New York City. “What a strange experiment I had conducted!” he notes.
Interwoven in the narrative of Jauhar’s new book, where the human drama of “doctoring” is leavened with biting observations and occasional humor, are his candid thoughts on the health care system, some of which he shares in the following interview. The second part of this feature is an exclusive excerpt from Doctoring. While Jauhar’s gaze can be withering, sparing not even family members, or indeed himself, he also has praise for dedicated professionals who make medicine, despite everything, a noble calling. And his passion for it is apparent.
Some readers will find Jauhar’s “money worries” jarring, given his qualifications (he also has a Ph.D. in physics from UC-Berkeley!) and his privileged status as a cardiologist at a well-known hospital. At times, this preoccupation in a section of the book threatens to confirm the stereotypical image people may have of “moneyminded” doctors.
“Live within your means,” his immigrant father admonishes. “And try to be happy.”
Yet it’s Jauhar’s bracing willingness to engage in honest, unwavering scrutiny that makes his book so readable. Doctors come in all types—quoting an economist, Jauhar describes them as a mix of knights, knaves, pawns— and there’s a disconnect, he notes, in how the public sees medicine and how physicians experience it from the inside. There’s a problem, too, in how the public views physicians, because they’re neither unrealistically selfless nor opportunistically greedy.
“What redeems the effort?” asks Jauhar, referring to his career choice. “It’s the tender moments helping people in need. In the end, medicine is about taking care of people in their most vulnerable state and making yourself a bit of the same in the process.”
Medicine touches our lives like no other profession. No wonder we continue to have such a high regard for it.
“I try to raise the issues that many doctors feel
is wrong with the profession.”
—Sandeep Jauhar
You’ve said that medicine has entered
a midlife crisis, and in your book
you take pains to spell out your disenchantment.
If you’d known this when
you were starting out, would you have
become a physician?
I think if I had known about all the
aspects—of course I had an inkling—I’d
have had second thoughts about becoming
a doctor. That’s not to say that
people go into medicine for the socalled
rewards. Today, medical practice
is so encumbered with paperwork,
malpractice fears, and so much waste,
it can be very disenchanting for a new
physician, someone who has different
expectations than what they see
when they enter practice. Clearly,
my ideals of what constituted good
medical practice were subverted in my
first few years as a physician—and that
was very disheartening.
Was becoming a doctor expected
of you when you were growing up?
You’re also a writer, of course, and
you have a Ph.D. in physics. So I’m
wondering when you got interested
in medicine. Or was it a question of
family pressure?
Well, family pressure certainly
played a role. My father came from
Kanpur and was very poor. He pulled
himself up by the bootstraps and became
a scientist. We lived on a scientist’s
salary. My father and mother both
wanted my brother and me and my
sister to become doctors to break out
of that. They came to the United States
with no money, no job security, nothing.
For them it was a constant struggle.
They had this sense that if you become
a doctor, you’ll achieve financial security
and job security. If I were
to become a scientist,
like my father, then I’d
always be vulnerable to
other people deciding on
my job status. In medicine,
you can always put
up a shingle, in their
view, and practice. There
was always a sense that
it’s a good profession, a noble profession.
You help people, and at the same time
you can do well by doing good.

(Left) Jauhar with a patient. “Most of us went into medicine to help people, not to follow corporate directives or even to maximize income,” he points out. “We want to practice medicine the right way, but too many forces today are propelling us away from the bench or the bedside.”
Your two books make for sober
reading; they’re cautionary tales. What
advice would you give to young Indians
who are contemplating a medical
career, or are already pursuing one?
Clearly, both books together are
a warning or a cautionary tale about
American medicine. However, I can tell
you that from my hard vantage point,
I’m very happy I became a doctor. Of
course, every day is a challenge—there’s
a lot of work, a lot of paperwork, and reimbursements
are cut so that you have
to see more patients to maintain your
income. It can be very hard, but at the
same time I feel very satisfied. One of
the reasons I feel satisfied is because in
addition to being a doctor, I found something
else that can absorb my energy.
And I think that’s very important going
into medicine, because if you devote
yourself to medicine to the exclusion of
everything else, you’re apt to burn out.
It’s very important to maintain some interest,
some outlet, whether it’s in your
family, sports, writing, whatever.

Sandeep and Sonia Jauhar with their children. His latest book is not just about medicine’s mid-life crisis; it’s also about his struggles to find balance as a middle-aged doctor, husband, and father.
In your books and sometimes in
your articles, too, you write quite frankly
about your family members—your
wife, your brother, your father, your
father-in-law. I’m wondering what the
reaction is like among them. Do you
discuss things in advance?
I don’t, but they generally have
been very, very supportive. My brother,
even though I may poke a finger at him
or criticize him, knows that he is one of
my heroes.
Which comes through in your
book. He was a great influence. He is a
rainmaker, but he is different. How was
your relationship when you were growing
up? Was it close?
I’d say it was close. But our personalities
are very different; we were also
very competitive with each other. We
wanted to outdo each other in tennis…
well, really, I wanted to outdo him. Because
I was so focused on doing better
than him, it propelled me to do better.
In a lot of things I probably edged him
out because I was more competitive. In
social relations, in knowing people and
being connected and having friends, he
was clearly superior and he knew it. And
that’s really served him well in life. My
wife—she has been very, very supportive.
She knows how much I value our life
together and our relationship.
And she is also a doctor. You talk
about how overutilization makes
our health care system dysfunctional.
The figure you state is $750
billion annually in wasteful spending.
There are many reasons for that,
but you say the biggest factor is the
fee-for-service model. Why do you
think it’s such a big problem, and how
can we address it?
The fee-for-service
model encourages
doctors to order
more tests because the financial
incentive is to
reward increased volume.
It’s essentially a
model that reimburses
doctors’ piece work.
So it encourages very
busy afternoons in the office—
patient visits every
10 minutes, a lot of tests.
And I think that contributes
to overutilization. There are
other factors—malpractice
worries, lack of time, being
rushed. You end up ordering
tests, ordering expert
consultations…you just don’t
have time to think through a case.
I wrote about that in The New York
Times. I think the models are now
slowly shifting towards pay-for-performance
or bundled payments. There
are different models in play that will
reward doctors not for how much they
test but for how well they perform.
That is generally a good thing, though
we have to do more work in defining
what is good care. That’s the challenge.
You point out that the medical field,
among all professions, has the highest
suicide rate. And you say that doctors
don’t seem to acknowledge that some
of it is caused by their own behavior.
Do you think they’re not facing up
to the burnout that’s inherent in the
profession?
That’s part of it. One of the main
reasons for the burnout has been the
increasing commercialization of medicine,
the business aspect of it that has
become so important. It has created a lot
of anxiety in the profession and doctors
have to look at themselves in the mirror
and understand why that is happening.
It’s not just insurers or the government
that is making doctors into businessmen;
it’s doctors themselves. If you look
at the history of American medicine,
there was a lot of waste and overutilization
engendered by the aspect of Medicare.
So doctors were responsible. Their
income went up nearly five-fold from
just before World War II to 1997. There
was a lot of waste and that led to a backlash.
That’s what led to managed care,
which put all the constraints into play—
all the paperwork and preauthorization
and all that stuff.
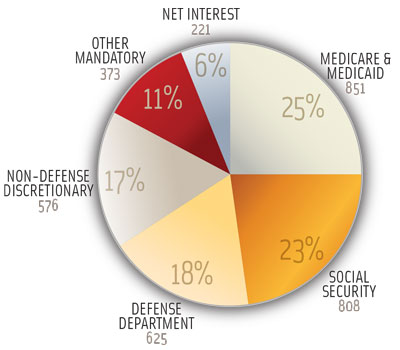
(Left) U.S. Federal Spending — Fiscal Year 2013 ($ Billions)
Total $3,454
Our ballooning medical costs are
unsustainable, Jauhar warns, and
shortchange crucial sectors like
education and infrastructure. We
may soon be spending 1 out of
every 5 dollars on health care.
What do you think of the Affordable
Care Act (aka Obamacare)—because
that’s supposed to fix some of the
problems, right?
I don’t think it does enough to bend
the cost curve, but it’s a step in the right
direction, because the systems that
we’ve been on are unsustainable. They
crowd out other very important spending—
on education, on infrastructure—
we need to do. We can’t spend all our
money on health care. Right now 1 out
of every 6 dollars in America is spent on
health care. Soon it’s going to be 1 out
of every 5 dollars…that’s way too much.
You’ve said that medicine is so
commercialized that private practice,
if one is not careful, can be corrupting.
You’ve written how some doctors are
unscrupulous or greedy, and you mention
how some doctors got together and
complained to your boss. So have you
suffered a backlash, professionally and
personally, because of your writing?
A lot less than one would think.
Doctors generally, my colleagues
[specifically], have been supportive
of my writing because I also put
the lens on my doubts and my own
behavior. People generally don’t
get upset when you accept blame for
your own foibles. I don’t try to point
the finger at other people. I try to raise
the issues that many doctors feel is
wrong with the profession. Generally
speaking, most physicians agree with
the bulk of what I say. And my views
have also evolved over time. In the past
I may have been a little more critical
of physicians; now I feel I have a more
nuanced view, that the whole system
is dysfunctional. It’s not just the physicians’
fault. All these different actors
in the system—government, insurers,
physicians, patients—are pursuing their
own end and leaving the system more
and more weak.
One of the more poignant stories
you tell is about Lily Dunhill, the elderly
woman you took care of and became
attached to. But it ended badly. Trying to prolong her life was a bad decision, because she suffered unnecessarily before dying. Can you talk about
self-deception, which seems to cost
us in more than one way? Is this a
major problem, especially in end-of-life situations?
Yeah, I think end-of-life is very
complicated. There are a number of factors that play a role in trying to get time to keep death at bay. Sometimes it’s the patients’ choice…they refuse our care. A lot of times it’s a family member’s choice—unwillingness, literally—to let go of a parent who’s entered the terminal phase of their disease. Traditions also play a role.
| “This lady was almost 90 years old and I put her in the ICU and started doing all these invasive things in a futile effort to save her.” |
With Lily Dunhill, I desperately wanted to save her. She was a very dear patient of mine and even in the face of what was going to happen—it was obviously going to end badly—I did all I could to see if we could potentially save her. It was only after that I thought, what did I really do? This lady was almost 90 years old and I put her in the ICU and started doing all these invasive things in a futile effort to save her. So I realized after the fact that it was full of folly. There was a degree of self-deception, but there were many different factors.
When is it okay to lie to a patient? You’ve addressed this.
I don’t think it’s ever okay to lie to
a patient per se. My [New York Times] op-ed was more about paternalism. Informed consent—and patient autonomy sometimes—seems to be so preeminent, but sometimes it’s possible that the doctor knows best. I think that exercising the soft kind of paternalism—where you encourage, control, communicate with the patient—is preferable in some cases than putting the entire burden of decision-making on a patient who
is sick. Sometimes patients end up
making what could clearly be the
wrong decision.

Speaking of op-eds, your piece on nurses drew a strong response. Some people argue that given the shortage of primary care physicians, it would be a good idea to use well-qualified nurses to fill a critical need in basic medical care. It also cuts costs. But you’re saying that this two-tiered system is neither wise nor fair. How do you respond to those who say, “Well, that’s doctors defending their turf.”?
I think for a lot of what’s fairly routine, for straightforward algorithmic care, it’s totally fine to have nurses or nurse practitioners acting fairly independently. But if there’s the occasional symptom that actually indicates cancer or something that’s unusual, that’s where you need a doctor’s expertise—because doctors have been trained over many, many years to have that clinical sense, that clinical acumen. And there’s no shortcut for developing that. We want to encourage medical students to go into primary care. Right now they’re not doing that because a lot of medical students are leaving medical school with $200,000 in debt. So they opt for higher-paid specialties. And primary care is also very difficult to deal with. You get paid to leave. It’s one of the most difficult fields…it has the most paperwork and so on.
You work in cardiology, which has seen dramatic improvements in patient care in recent decades. But that has slowed recently. You say that now we should shift our focus from ‘door-to-balloon’ to ‘symptom-to-door.’ How will this improve cardiac care?
Right now the focus for treating heart attacks is on what’s called door-to-balloon time. How long it takes from arrival at the ER to putting in the stent to open up the blockage—that’s called balloon time. But before patients even arrive in the hospital, there’s often a
very long time lag. Patients ignore their
symptoms, they may be ignorant that
they’re having a heart attack. So what I
say is maybe symptom-to-door time is
more important, because door-to-balloon
time is a relatively small fraction of
the total time the patient is having the
heart attack. If we encourage patients
to come to the hospital faster, we also
encourage ambulances to take patients
to the right—not the nearest—hospital,
where they do angioplasty and have a
cardiac catheterization lab.
Finally, have you come to terms
with your profession? It looks like, despite
all the criticisms, you like being a
cardiologist.
I enjoy coming to work, treating patients.
That’s the best part of my job…it’s
developing relationships with patients,
seeing them and spending time with
them, and being part of their lives. So to
me that’s the underpinning of my professional
passion.
Part 1: Ambition, Chapter 1: Awakening
By SANDEEP JAUHAR
A young doctor means a new graveyard. —German proverb
I had been pedaling furiously for nearly a decade —on a stationary bicycle. Medical school, internship, residency, and fellowship: my education seemed as if it would never end. So it was with no small measure of relief that in the late spring of 2004 I accepted a position as an attending cardiologist at Long Island Jewish Medical Center in New Hyde Park, New York. This was the last step in a long and grueling journey. After medical school I’d completed three years of hospital instruction in general internal medicine to earn the privilege to practice independently. After finishing this internship and residency, I’d elected to do a fellowship: three more years of study in cardiac diseases to further specialize. Now, with the fellowship concluded, I’d become an attending physician, the senior level of the hospital hierarchy, with ultimate responsibility for patients and junior doctors. Nineteen years after starting college and a few months shy of my thirty-sixth birthday, I finally had my first real job. The complexities of academic medical training had long since worn thin. I was ready to simplify, consolidate, and perhaps even reap some rewards for all those sleepless nights.
Cardiology was a natural career choice. I had trained as a physicist before going to medical school, and the heart, with its complex rhythms and oscillations, appealed to my predilection for patterns and logic. Heart disease was also no stranger in my family. Both my grandfathers had died of myocardial infarctions—one in his forties, ten years before I was born—so I had grown up with an awe of the heart as the executioner of men in the prime of their lives. Plus, the heart, with its symbolic meanings, had always occupied a special place in my (and the broader cultural) imagination. Take heart! Have a heart! He wears his heart on his sleeve.
Of course, I was nervous. Every new doctor should be. Cardiologists specialize in emergencies. The culture is fast-paced, pressured. I was going to have to learn to become quick and decisive in precarious situations. By nature I was slow and deliberate, and I had never felt comfortable acting on instinct—not exactly adaptive in a cardiac care unit where people can drop dead on you at any moment. In neuroscience there is the concept of the reflex arc, in which a threatening stimulus can effect a response without passing through the conscious brain—for example, when you see the taillight flash red on the car speeding in front of you and your foot automatically moves to the brake pedal. I was afraid that as a cardiologist I would now have to follow a similar reflex arc.
“Well begun is half done,” my father reminded me with his usual Aesopian wisdom. Dad possessed the annoying certitude that there were no more life lessons to be learned in this world, that whatever was worth knowing our forebears had already taught us. Traditional and moralistic, he liberally quoted proverbs and scriptures even if he didn’t always live by them. But when you think in axioms and parables, when the collective wisdom of the world can be distilled into the concentrated tonic of a few sayings, then you feel as though you have all the answers.
He had always wanted me to become a doctor— one trained at Stanford University, no less. That, he believed, would be the pinnacle of professional attainment. My family immigrated to the United States in 1977, when I was eight, to advance my father’s career as a plant geneticist, but in America my father never achieved the kind of success he felt he deserved—denied, he believed, by a racist university tenure system, which forced him to take postdoctoral positions with no long-term stability and left him embittered and in a constant state of conflict with professional colleagues. In medicine, my father explained, I would not be plagued with such insecurity.
One reason for my father’s struggles was that he always seemed to do things the wrong way. When I told him the mnemonic I had learned in school to remember the colors of the spectrum, he said: “Roy G. Biv? Oh, you mean Vibgyor!” He’d mow the lawn at night, waking the neighbors. He’d bring up controversial subjects like Sikh separatism or Kashmiri violence at low-key social gatherings. He’d trim our nails with a Gillette razor blade, twisting our fingers painfully so they wouldn’t get lacerated. As long as the nails got cut, it didn’t matter to my father how much we protested. That sort of encapsulated his personality: disciplined, unsentimental, focused solely on the task at hand.
| “She often told us she wanted her children to become doctors so people would stand when we walked into a room.” |
My mother affectionately called him poottha, “awkward.” She accepted his idiosyncrasies with a kind of bemused resignation, as if they had been written in the stars. The eldest daughter of a wealthy New Delhi physician, she abided her station as the working wife of a discontented plant geneticist as though it had been ordained, just part of the deal of an arranged marriage, and she resolved to make the most of it. She didn’t believe in talk or analysis or drama, only in putting your best foot forward and grinding ahead, accepting your circumstances with dignity and grace. Yet for all her equanimity, she still regarded medicine as the hammer that would break her children out of the middle-class mold my father had set. She often told us she wanted her children to become doctors so people would stand when we walked into a room.
My apprehensions about my new job were only slightly mitigated by the fact that my older brother, Rajiv, an interventional cardiologist who performed invasive procedures, was already working at the same hospital. Rajiv was my parents’ firstborn, their pride. They had always favored him, and Rajiv demanded it, too. He knew the privileges of being the elder son in a traditional Indian family and guarded them closely, like a trust fund. Like most brothers close in age, we were fiercely competitive growing up, evenly matched at most things (ping-pong, chess, tennis), our rivalrous parity enforced by the unspoken fear that if one of us pulled away, we’d lose the other’s companionship. One sphere in which we were undoubtedly unequal was social relationships, however. Rajiv had the kind of gregarious and easygoing personality that I had always desired but somehow never could develop. The only time we had worked together professionally was during my internship at New York Hospital in Manhattan, where as a star senior cardiology fellow he unwittingly reminded me of my incompetence again and again. Toward the end of my own cardiology fellowship at NYU, he had invited me to apply to LIJ and had used his considerable influence to get me a job. Now he was in a position to guide me through another, perhaps more challenging apprenticeship.
At Long Island Jewish I would work as a cardiologist with a specialization in congestive heart failure. This was no small task: heart failure is the common final pathway for a host of cardiac diseases, including heart attacks, acute valve disorders, viral infections of the cardiac muscle, etc. There are many challenges in caring for these patients. They have multiple comorbid illnesses, such as diabetes and emphysema. Their symptoms—for instance, shortness of breath— are often nonspecific. They frequently have poor health literacy or cognitive impairment or are socially isolated because of their chronic disease. Despite these difficulties, I chose to specialize in heart failure because I wanted to develop close relationships with critically ill patients and provide long-term care, unlike my brother, who almost exclusively performs procedures and knows his patients mostly for the duration of an operation. I also wanted to be in a specialty where I would not have to perform surgical interventions. I’d never been especially good with my hands. Growing up, Rajiv had been the tinkerer and I had been the thinker. Of course, I knew this decision was going to involve a certain degree of monetary sacrifice. Heart failure is a money loser for most hospitals, which make most of their revenue from lucrative procedures like stents (wire mesh cylinders used to open blockages in the coronary arteries that feed the heart) and pacemakers, or hip replacements. In the American system doctors are paid much less for exercising their judgment than their fingers.
Reprinted from Doctored: The Disillusionment of an American Physician with the permission of Farrar, Straus and Giroux, New York.
Enjoyed reading Khabar magazine? Subscribe to Khabar and get a full digital copy of this Indian-American community magazine.






